
VERTEBRAL COMPRESSION FRACTURE
Proliance Orthopedic Associates



ABOUT THIS CONDITION
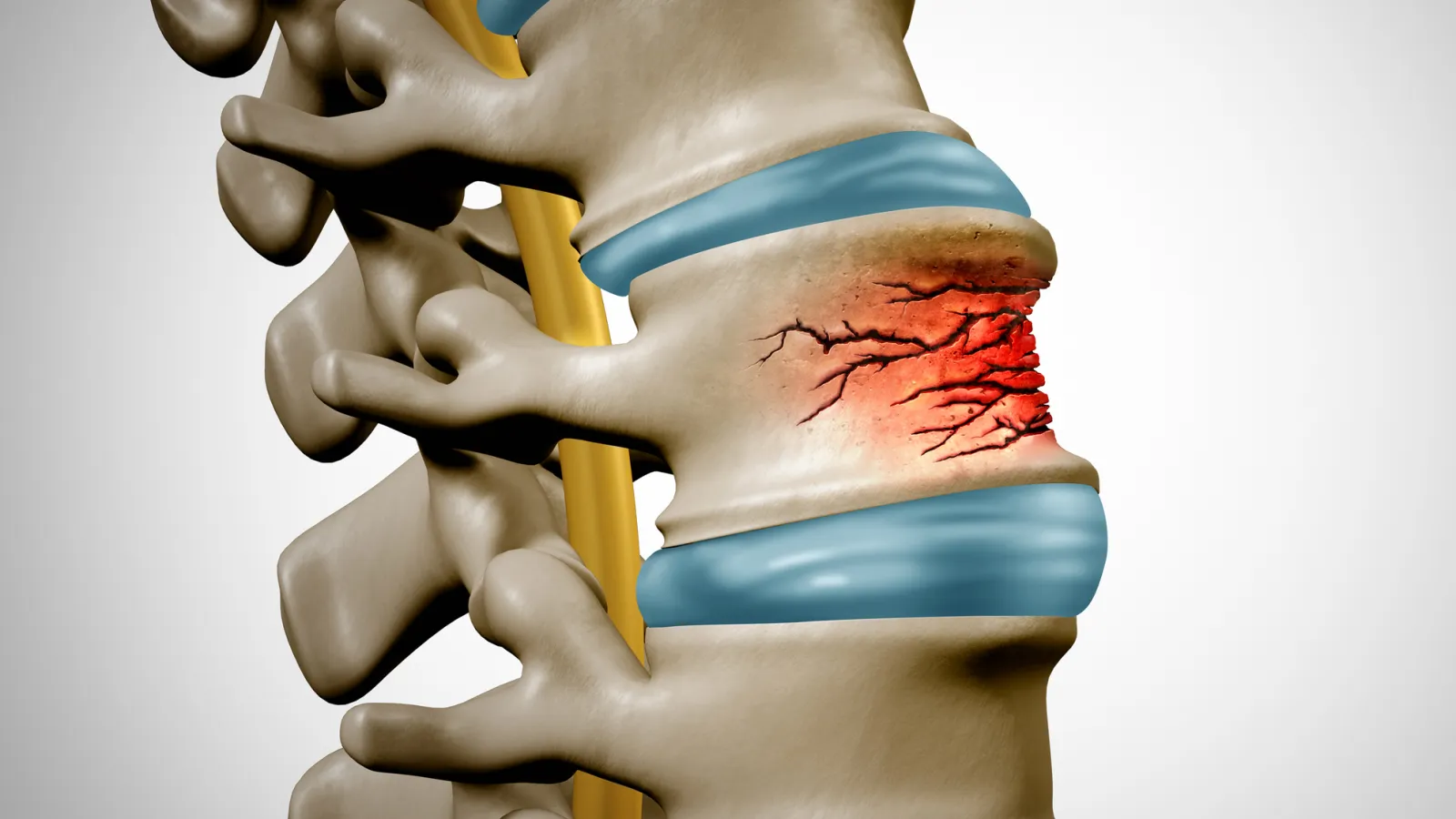
A vertebral compression fracture occurs when a vertebral body in the spine collapses or cracks, losing height. These fractures most commonly occur in the thoracic spine (mid- back) and the thoracolumbar junction (where the mid-back meets the lower back). They are one of the most common fractures associated with osteoporosis.
In patients with osteoporosis, the bones are weakened to the point where even minimal force — bending over, lifting a light object, or even coughing — can cause a vertebra to fracture. In patients with normal bone density, compression fractures result from higher- energy trauma such as falls from a height or motor vehicle accidents. Compression fractures can also occur in patients with cancer that has spread to the spine (pathologic fractures).
Symptoms include sudden onset of back pain that worsens with standing and walking and improves with lying down. The pain is usually localized to the area of the fracture. Over time, multiple compression fractures can lead to progressive loss of height and a stooped or rounded posture (kyphosis). Some patients also experience radiating pain around the rib cage or abdomen.
Vertebral compression fractures are extremely common — approximately 700,000 occur annually in the United States. They disproportionately affect postmenopausal women, elderly adults, and patients on long-term corticosteroid therapy.
TREATMENT
Most vertebral compression fractures are treated non-surgically. Dr. Daniel Oh manages these injuries at our Renton and Covington locations with a comprehensive approach that includes pain management with medications, a short period of rest followed by early mobilization, and bracing to support the spine and reduce pain during healing. Walking and gentle activity are encouraged as soon as pain allows, as prolonged bed rest leads to deconditioning and further bone loss.
Treatment of the underlying osteoporosis is essential to prevent future fractures. This includes ensuring adequate calcium and vitamin D intake, bone-strengthening medications (bisphosphonates, denosumab, or teriparatide), fall prevention strategies, and regular bone density monitoring.
For patients with severe, persistent pain that has not responded to conservative treatment after four to six weeks, a vertebral augmentation procedure may be recommended. Kyphoplasty involves inserting a small balloon into the fractured vertebra, inflating it to restore height, and then filling the space with bone cement to stabilize the fracture. This provides rapid pain relief in most patients and is performed as a minimally invasive outpatient procedure at Proliance Surgery Center at Valley in Renton.
RECOVERY
Most compression fractures treated conservatively heal within six to twelve weeks, with the majority of patients experiencing significant pain relief within the first four to six weeks. Return to normal activities is gradual and guided by symptoms. After kyphoplasty, pain relief is often immediate to within a few days, and patients can resume normal activities within a few weeks. Regardless of the treatment approach, long-term management of osteoporosis is essential to reduce the risk of future fractures. A structured exercise program that includes weight-bearing activity, balance training, and gentle strengthening helps maintain bone density and prevent falls.
FREQUENTLY ASKED QUESTIONS
Q What causes compression fractures?
The most common cause is osteoporosis — weakened bones that fracture with minimal force. In younger patients, compression fractures result from high-energy trauma such as falls or accidents. They can also occur in patients with cancer that has spread to the spine.
Q Will my compression fracture heal on its own?
Yes. Most compression fractures heal with conservative treatment within six to twelve weeks. Pain management, bracing, and early mobilization are the cornerstones of treatment.
Q What is kyphoplasty?
Q How can I prevent future compression fractures?
Treating the underlying osteoporosis is the most important step. This includes calcium and vitamin D supplementation, bone-strengthening medications, regular weight- bearing exercise, fall prevention strategies, and regular bone density monitoring.